Research Snippet 6: Melanoma in Australia
Epidemiology of Melanoma
Just 30 minutes. It may seem like such a short amount of time but every 30 minutes, one person is diagnosed with melanoma in Australia [1]. Australia has a high incidence and prevalence of Melanoma, with it being the third most common cancer in both males and females [1]. Though melanoma is the deadliest skin cancer, it is said the risk of diagnoses at age 30 has halved since 1997. [1,2].
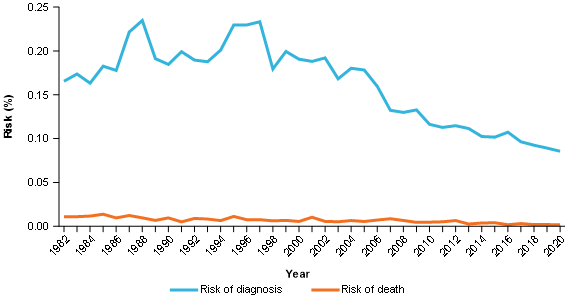
Figure 1: Incidence and mortality risk by the age of 30, melanoma of the skin, persons
Note: Incidence risk for 2017–2020 and mortality risk for 2019 – 2020 are based on projections.
Source: AIHW Australian Cancer Database 2016 and National Mortality Database
However, though the risk of incidence at age 30 has decreased, and the risk of diagnosis at age 60 continues to be stable since 2012, the lifetime risk of melanoma has more than tripled since 1982. Given this information, it is most likely due to the older population and increased life expectancy. In other words, improved living conditions and life expectancy means that more people are living to an advanced age when melanoma is more common to be diagnosed.
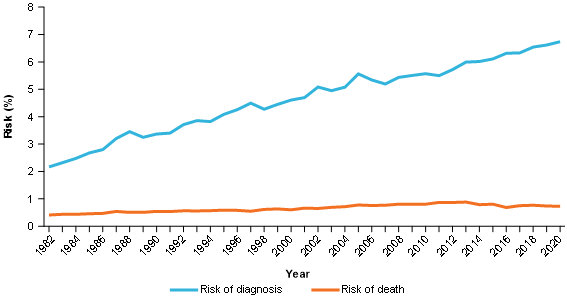
Figure 2: Incidence and mortality risk by the age of 60, melanoma of the skin, persons
Note: Incidence risk for 2017–2020 and mortality risk for 2019 – 2020 are based on projections.
Source: AIHW Australian Cancer Database 2016 and National Mortality Database
In Australia, there are a number of risk factors for the diagnosis of melanoma including: fair complexion, excessive sunlight exposure, history of blistering sunburns, age >50, and a family history of atypical moles or melanoma [3]. Melanoma is also more common in men than women in Australia [4].
Usually, the first sign of melanoma is the appearance of a new lesion on the skin or the evolution of a pre-existing mole. There tend to be gradual changes in the melanoma over time including size, shape and colour [4]. If you are unsure about any atypical mole on your skin, you should consult your doctor who will thoroughly inspect the suspicious lesion via a dermatoscope for asymmetry, border irregularities, colour, diameter, and evolution.
There are new innovative ways to treat melanoma and improve patient prognosis including immunotherapy and surgical techniques that we will delve into!
Melanoma Immunotherapy
Only a decade ago, metastatic melanoma was regarded as virtually untreatable. Such a grim prognosis was attributed to the relative ineffectiveness of traditional chemotherapeutic agents. Since that time, our fight against melanoma has come leaps and bounds. Today, state of the art Check-point Blockade Immunotherapies – which harness and augment the body’s own immune system – have transformed the treatment landscape for advanced melanoma, such that the 5-year survival rate is now well over half of all patients.
Interestingly, the basis of Checkpoint Immunotherapy was first discovered in the field of viral immunology. Some viral infections such as hepatitis viruses cause chronic long-term infections, where neither the virus nor the immune system is able to get an upper hand. Typically, our immune cells get activated or boosted each time they encounter their target. In the case of a long-term infection, this leads to the dangerous possibility of our immune cells being repetitively “revved up”, to a point where they may damage our own body cells. To prevent such a situation, immune cells have natural inbuilt brakes called “checkpoint inhibitor” receptors such as PD-1 and CTLA4. The consequence of these brakes, is that with repetitive encountering of the virus, immune cells instead get down-regulated in their activity, to a level JUST ENOUGH to keep the virus in check, while minimising immune-mediated damage to the host.
The serendipitous link into the field of Oncology, came with the later discovery that that tumour-specific immune cells also often express those same inhibitory checkpoint receptors – CTLA4 and PD-1, suggesting a similar dynamic where immune cells are repetitively encountering cancer cells. Hence, researchers came up with the idea to treat cancer by blocking these CTLA4 or PD-1 interactions with specifically designed monoclonal antibodies [5]. The result was akin to “releasing the brakes’ ‘; with the effect of reinvigorating the immune response against Melanoma. For their novel approach and groundbreaking contribution to the field of Cancer Research, the lead scientists Jim Allison and Tasuko Honku were awarded the 2018 Nobel Prize in Medicine.
And yet, despite how far we’ve come, there is clearly room for improvement. Jim Allison’s and Tasuko Honku’s work paved the way for other scientists to explore the complexity of immune-modulating receptors. As new checkpoint inhibiting molecules are discovered, there is increasing promise of combination therapies. But there still remains the perplexing fact that not all patients with melanoma respond in the same way to checkpoint blockade therapy. Scientists are only now beginning to tease apart the individual-specific factors which affect prognosis; an exciting intersection between the fields of cancer immunotherapy and personalized medicine.
Melanoma Surgical Techniques
Whilst medications and radiation therapy may be effective for a number of patients, given the aggressive nature of Basal Cell Carcinomas (BCC’s) and Squamous Cell Carcinomas (SCC’s) surgical resection is recommended in combination with pharmacological therapies. Whilst certain procedures may appear simple on the surface, the nature of surgical resection often depends on the stage and grade of the skin cancer, with procedures ranging from simple curettage to complex cases requiring an interdisciplinary team. The main surgical techniques include electrodesiccation and curettage, standard surgical excision, Mohs surgery and more complex reconstructive cases.
Simple curettage is performed on both small BCC’s and SCC’s that have not invaded beyond the superficial layer of the skin (nor in sensitive areas). This often involves simple scraping of cancer cells from the epidermal layer of the skin and electrodesiccation (applying a small amount of electricity to the area) to prevent bleeding [6]. Overall, this technique is performed for low grade, well-demarcated carcinomas and has a great patient outcome, as it prevents many from going under general anesthesia or into more complex surgical cases. One major downfall however is the lack of a specimen at the end of the procedure – this means that oftentimes physicians cannot be certain of what type of cancer was removed and further investigation is required [6].
Moreover, standard surgical excision involves the removal of the entire tumour that has penetrated beyond the epidermal layer. Often performed under local anesthetic this technique has great success post-surgery. Mohs surgery (also known as micrographic surgery) is a surgical technique that goes beyond simple surgical excision. Mohs surgery is often considered the front-line gold standard treatment for non-melanoma skin cancers or for patients who have had recurrence of a previously treated skin cancer [6]. The major difference between standard surgical excision and Mohs surgery is the timeline – Mohs surgery is performed in stages, from surgical excision to histopathological/microscopic analysis all completed by the same surgeon and on the same day [6]. This continuity of care ensures that the surgeon is able to more precisely and accurately excise all of the cancerous cells in one surgery. All of this is often performed on extremely visible areas so surgical prowess is paramount to ensure minimal scarring.
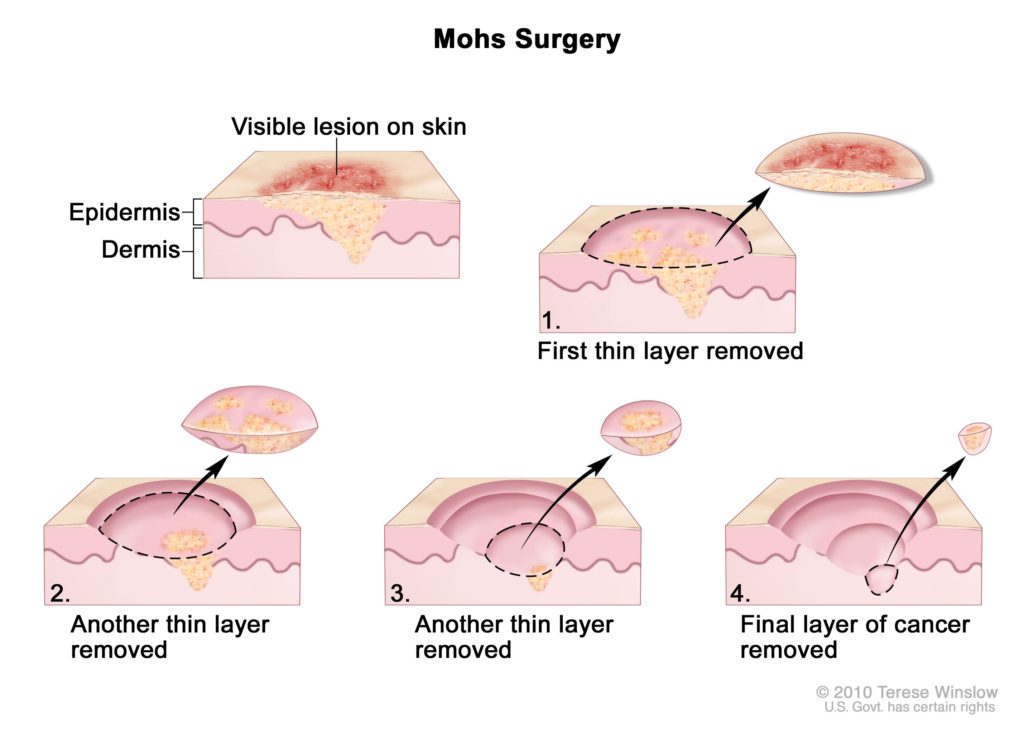
Figure 3. Illustration of Mohs surgery.
NCI Dictionary of Cancer Terms. (2021). Retrieved 1 June 2021, from https://www.cancer.gov/publications/dictionaries/cancer-terms/def/mohs-micrographic-surgery
Finally, more complex surgeries for skin cancer may also involve reconstruction of the area following surgical excision. This is used for skin cancers that have penetrated deeper into the skin layer. Reconstructive cases can range from simple skin grafts where healthy tissue from another part of the body is grafted onto the area where the cancer was removed to more complex free rotational local flaps (where tissue along with its own blood supply is precisely excised and grafted onto the previous cancer site and left to grow).
Future Remarks
To continue to improve melanoma outcomes, there has to be an increased focus on early detection through regular screening, increased awareness of the risk rates and finally a personalised approach to treatment. These include targeting high-risk individuals based on epidemiology such as those above 60, as well as high UV radiation areas in Australia. Through these means, early diagnosis and identification of melanoma can have immense benefit to reducing overall costs to the health system. Below is an image that captures this process:
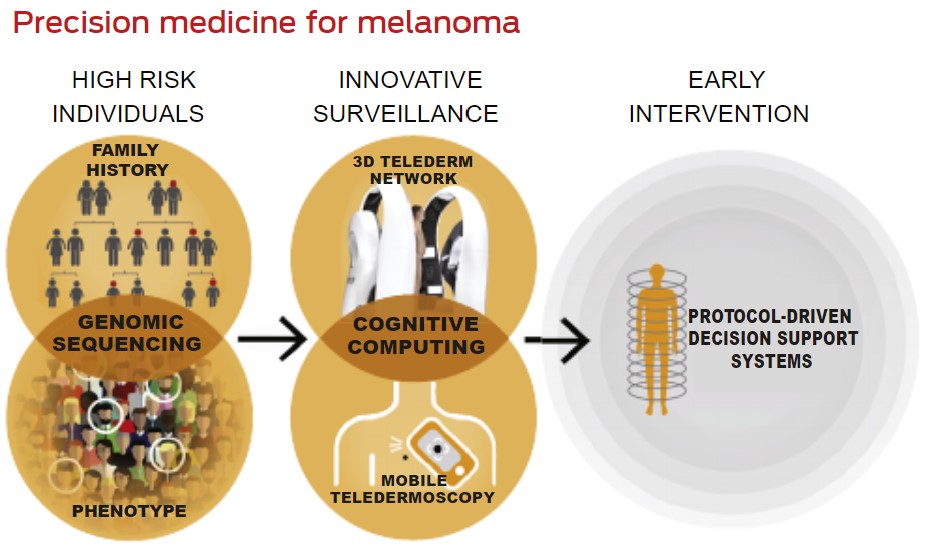
Figure 4. A personalised approach for melanoma management incorporating risk stratification and innovative surveillance for early intervention.
Taken from: Whither melanoma in Australia? Medical Journal of Australia [7]
References
[1] Melanoma facts and statistics [Internet]. Melanoma Institute Australia. [cited 2021May31]. Available from: https://www.melanoma.org.au/understanding-melanoma/melanoma-facts-and-statistics/
[2] Cancer data in Australia, Risk of melanoma of the skin by age and over time [Internet]. Australian Institute of Health and Welfare. [cited 2021May31]. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia/contents/cancer-data-commentaries/risk-of-melanoma
[3] Cancer Australia. What are the risk factors for melanoma? [Internet]. What are the risk factors for melanoma? | Cancer Australia. Cancer Australia; 2019 [cited 2021May31]. Available from: https://www.canceraustralia.gov.au/affected-cancer/cancer-types/melanoma/what-are-risk-factors-melanoma
[4] Melanoma Diagnosis [Internet]. Alfred Health. [cited 2021May31]. Available from: https://www.alfredhealth.org.au/services/statewide-services/victorian-melanoma-service/melanoma-treatment-options/melanoma-diagnosis
[5] Waldman, A., Fritz, J. and Lenardo, M., 2020. A guide to cancer immunotherapy: from T cell basic science to clinical practice. Nature Reviews Immunology, 20(11), pp.651-668. Available from: https://www.nature.com/articles/s41577-020-0306-5
[6] Rogers-Vizena, C., Lalonde, D., Menick, F., & Bentz, M. (2015). Surgical Treatment and Reconstruction of Nonmelanoma Facial Skin Cancers. Plastic And Reconstructive Surgery, 135(5), 895e-908e. doi: 10.1097/prs.0000000000001146.
[7] Smithers BM, Dunn J, Soyer HP. Whither melanoma in Australia? Medical Journal of Australia. 2017;207(8):330–1.


